How Can We Better Classify Neurorehabilitation?


Want to listen to this article for FREE?
Complete the form below to unlock access to ALL audio articles.
Read time: 4 minutes
Neurological disorders affect a significant proportion of the population1 and approximately 47% of individuals have concurrent mental health issues2. These shocking statistics highlight the necessity for a strong framework for conceptualising neurological health conditions.
The International Classification of Functioning, Disability and Health
The International Classification of Functioning, Disability and Health (ICF) conceptualises neurological conditions at three core levels3 (see image 1). The ‘Health condition’ refers to the individual’s clinical signs and symptoms. ‘Body structure and functions’ refers to the functional capacity of one’s bodily systems. ‘Activity’ and ‘participation’ refer to one’s involvement in various daily activities. At the third level, there are contextual factors, including environmental and personal facets that may influence recovery; these contextual factors can either assist or impede recovery.
Moreover, the ICF has four key underlying philosophical principles. Firstly, the ICF aims to be applicable to everyone across all socio-cultural contexts. Secondly, the framework focuses on the individual’s ability to engage in meaningful activities, rather than their physical ‘deficit’. Thirdly, the ICF uses neutral, non-judgemental language. Finally, this framework places greater emphasis on the influence of environmental factors on neurorehabilitation, referring to meaningful improvements in functioning that maximise one’s ability to engage in desired activities.
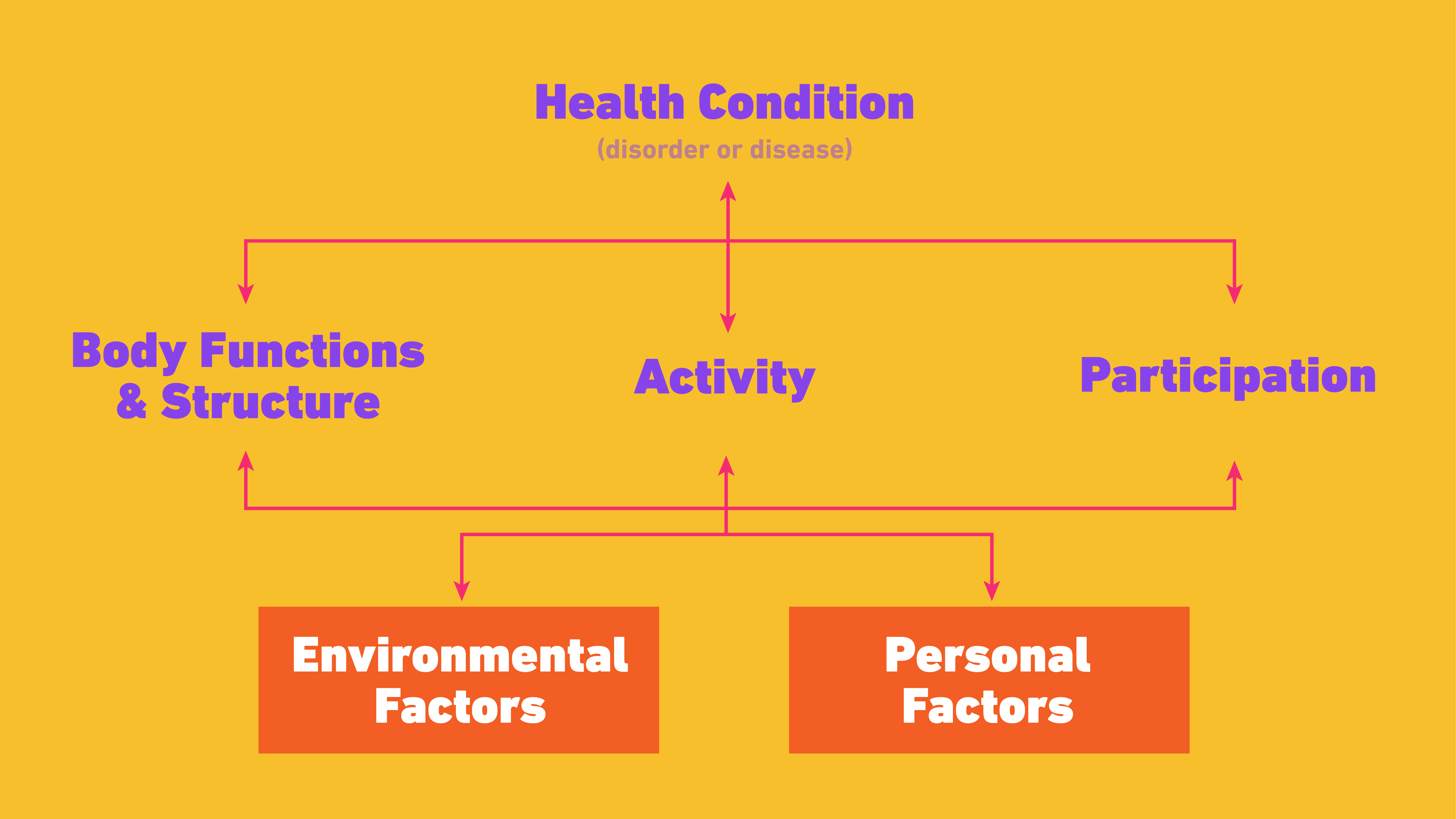
Image 1: The ICF framework.
Advantages of the ICF:
This framework represents a radical advancement on the previous International Classification of Impairments, Disability and Handicaps (ICIDH)4. Compared to the ICIDH’s narrow ‘medical model’ approach, the ICF argues that ‘disability’ is multi-factorial in nature, such that ‘impairment’ can occur at numerous levels. Importantly, this implies that recovery is also non-linear and can occur at biological, psychological, environmental and social levels5. This indicates that recovery does not necessarily have to occur at the physiological level, nor is it necessarily a regression to one’s former self prior to the impairment. Instead, recovery involves forging a new way of living that maximises the client’s ability to engage in activities and have a meaningful life.
One of the ICF’s most innovative changes relates to the acknowledgement of the influence of environmental factors on health conditions. The framework highlights that the person’s ability to function is only ‘impaired’ relative to the demands of their environment6, 7. For example, an individual with a reduced ability to climb stairs is only impaired in an environment that requires them to climb stairs. Accordingly, if they live in a bungalow, they are no longer impaired. This shift in conceptualising health conditions may seem relatively minor, however it entails the radical implication that clinicians can treat health conditions by altering the individual’s environment as well as their physiology.
Another practical improvement concerns the ICF’s exhaustive coverage of the aspects of functioning. Many assessment tools have been developed to assist clinicians in examining different levels of functioning. However, these extensive checklists can be time-consuming, which can have repercussions on the efficiency, welfare and performance of clinicians8,9. Nevertheless, the comprehensive list of functional capacities is highly useful for clinicians and helps to avoid clinical errors, such as failing to assess a specific aspect of functioning.
Limitations of the ICF:
Despite its innovative approach to neurorehabilitation, the ICF has some limitations. One of the major shortcomings relates to the distinction between ‘participation’ and ‘activity’. Whilst conceptually distinct, these aspects of functioning often have large practical overlap. This arises because one’s ability to participate in activities is often intertwined with their ability to undertake relevant physical actions. The practical overlap has resulted in differences between clinicians in the use of these constructs, with variation in the functional capacities classed as ‘activity’ and ‘participation’10. This inconsistency results in challenges when comparing data from different clinicians11.
Furthermore, the measures used to assess participation and activity rarely assess all aspects of functioning. Evidence for this comes from Chien et al (2014) who studied 16 measures of participation and reported that none comprehensively evaluated all aspects of participation12. Further evidence comes from Chang et al (2013), who evaluated the efficacy of participation measures for individuals who have had a stroke13. Again, they found that none of the measures provided a complete assessment of engagement with community activities. Evidence comparing these measures is also sparse, making it difficult to determine whether some tools provide better measures than others14. It is critical that comprehensive and standardised measures of both activity and participation are developed that can be applied to all demographics.
There are also numerous issues regarding the generalisability of the framework, particularly to children. Rune Simeonsson and colleagues noted that the influence of environmental factors is much greater in childhood than adulthood, as the environment shapes development, but the ICF fails to acknowledge this15. In addition, functional limitations that may be considered an impairment in adulthood are not necessarily classed as impairments in childhood. For example, Simeonsson et al (2003) highlighted that disruptions to sleep are very common in childhood and consequently would not necessarily be considered a health condition, whereas this is not the case in adulthood15. Future research is required to develop tools that can assess functional capacities from birth.
Another limitation relates to measuring the various aspects of functioning detailed in the ICF. Despite placing large emphasis on environmental factors, the ICF often fails to assess functioning in the client’s natural environment, instead relying on assessment in clinical settings. Overcoming this is not easy and many clinicians resort to asking the individual about their activity outside of the clinic room. However, memory is fallible, particularly for those with neurological conditions such as Alzheimer’s disease, casting doubt on the validity of such approaches. It may be useful to recruit the knowledge of others who spend time with the client, such as a family member, as they often observe functioning in a more natural context16.
The ICF entails a comprehensive list of ‘codes’, which describe different aspects of functioning. However, the measures used to assess functioning rarely have a direct correspondence to the specified codes in the ICF17. Multiple ICF codes often underlie a single question in assessments, which can result in difficulty when attempting to identify the precise aspects of functioning that are impaired. Moreover, whilst conceptually distinct, many of the codes have significant practical overlap. For example, Reed et al (2005) highlighted that the ICF distinguishes between ‘conversation’ and ‘discussion’ as two separate abilities and that, whilst conceptually distinct, this distinction has limited clinical implications17.
Concluding Comments:
In conclusion, the ICF represents a major leap forward in the way in which clinicians understand both neurological health conditions and neurorehabilitation. This framework represents a shift in conceptualising health conditions and takes greater account of how they are influenced by the socio-political environment. However, there are still many improvements to be made and future research will be vital for implementing these changes.
Meet the Author

