T-helper cell phenotype expression in cutaneous lesions of angioimmunoblastic T-cell lymphoma
Background:
Angioimmunoblastic T-cell lymphoma (AITL) is a common type of peripheral T-cell lymphoma. AITL can be missed until lymphadenopathy develops in patients initially presenting with skin lesions, as skin biopsy may lack conclusive findings. The expression of follicular helper T-cell (THF) markers in the skin can be an important diagnostic clue. We present a case of AITL with skin lesions positive for CD10 and dim PD1 T-cells, with the purpose of highlighting the potential for diagnosing cutaneous AITL via skin biopsy.
Case Presentation:
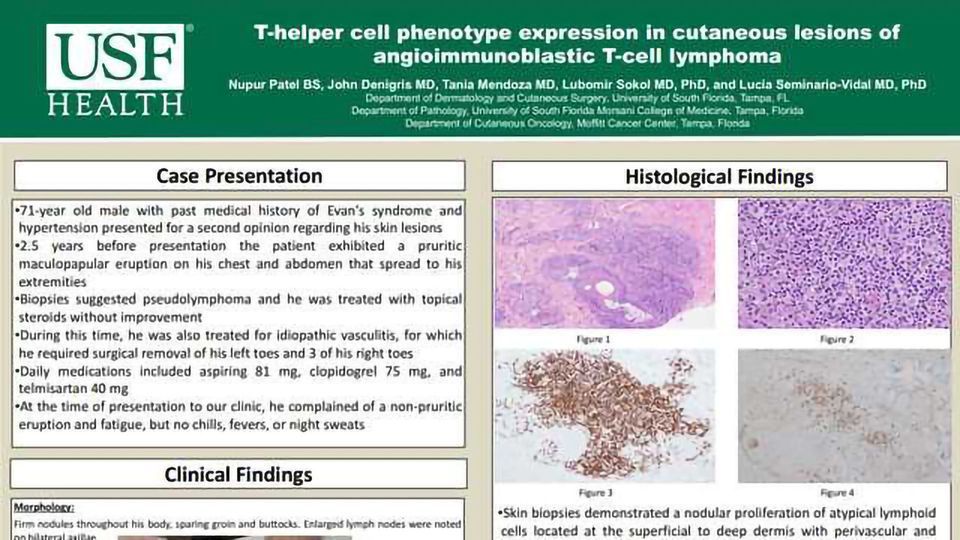
71-year old Caucasian male presented for second opinion of his skin lesions. On exam, there were firm nodules throughout his body with enlarged lymph nodes on bilateral axillae. Skin biopsies demonstrated nodular proliferation of atypical lymphoid cells with perivascular and periadnexal infiltration. Staining revealed more prominent B-cell lymphoproliferative, while limited T-cell infiltrate expressed TFH markers, CD10 and PD1, suggestive of TFH origin. Fine needle aspiration of lymph node revealed an aberrant T cell population. Peripheral blood flow cytometry and bone marrow analyses also identified abnormal T cell population with TFH phenotype. Based on overall findings and pathology, diagnosis of AITL was made.
Discussion:
Our case highlights the extranodal presentation of AITL with cutaneous lesions displaying the TFH phenotype. Although AITL and the presence of TFH markers is generally studied via lymph node biopsy, the disease often presents with prominent skin findings that can be diagnosed via biopsy. Further insight into markers specific for cutaneous AITL may lead to advances in diagnostic strategies and clinical outcomes of AITL.
Angioimmunoblastic T-cell lymphoma (AITL) is a common type of peripheral T-cell lymphoma. AITL can be missed until lymphadenopathy develops in patients initially presenting with skin lesions, as skin biopsy may lack conclusive findings. The expression of follicular helper T-cell (THF) markers in the skin can be an important diagnostic clue. We present a case of AITL with skin lesions positive for CD10 and dim PD1 T-cells, with the purpose of highlighting the potential for diagnosing cutaneous AITL via skin biopsy.
Case Presentation:
71-year old Caucasian male presented for second opinion of his skin lesions. On exam, there were firm nodules throughout his body with enlarged lymph nodes on bilateral axillae. Skin biopsies demonstrated nodular proliferation of atypical lymphoid cells with perivascular and periadnexal infiltration. Staining revealed more prominent B-cell lymphoproliferative, while limited T-cell infiltrate expressed TFH markers, CD10 and PD1, suggestive of TFH origin. Fine needle aspiration of lymph node revealed an aberrant T cell population. Peripheral blood flow cytometry and bone marrow analyses also identified abnormal T cell population with TFH phenotype. Based on overall findings and pathology, diagnosis of AITL was made.
Discussion:
Our case highlights the extranodal presentation of AITL with cutaneous lesions displaying the TFH phenotype. Although AITL and the presence of TFH markers is generally studied via lymph node biopsy, the disease often presents with prominent skin findings that can be diagnosed via biopsy. Further insight into markers specific for cutaneous AITL may lead to advances in diagnostic strategies and clinical outcomes of AITL.




