How Can Machine Learning Improve Surgery?

Complete the form below to unlock access to ALL audio articles.
Machine learning modeling is one of the most eagerly adopted technologies across healthcare. In their recent report, Accenture predicted that healthcare AI market value will reach $6.6 billion by 2021, mostly thanks to robot-assisted surgery. Indeed, AI’s rapid evolution will soon allow machine learning models to enhance the current surgical practice.
There are several stages of the process leading up to, during and after the surgical procedure where AI can lend a hand (or processor). Before performing a surgery, health specialists have to complete the decision-making and incision-planning phases. Sometimes, these phases require making difficult choices (multimodal therapy, radical vs. organ-preserving surgery, the best timing for the procedure, etc.). Besides, professionals may need to visualize the expected results, when it comes to aesthetic or reconstructive surgery.
Additionally, surgeons are expected to provide their patients with personalized suggestions on possible risks, health outcomes, and chances for full recovery. Patient-level predictions depend on multiple parameters beyond human abilities to connect, process, and employ. In most cases, health specialists and their patients will have to settle for average in-hospital morbidity, mortality, and recovery stats.
In this article, we will review current and upcoming applications of machine learning in burn surgery and microsurgery.
Burn surgery: assessment and planning
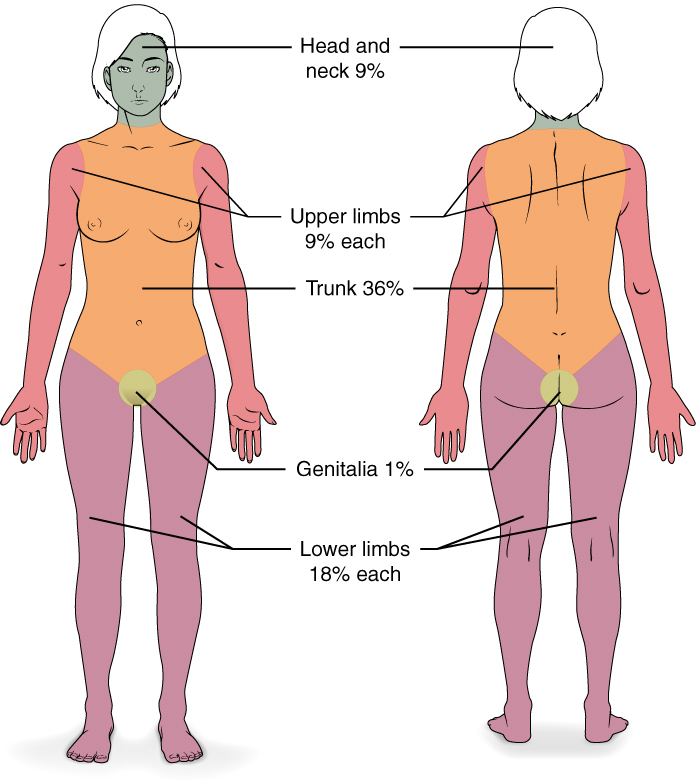
Doctors who treat patients with burns start by assessing the burned body surface area. For this, health specialists assume that a patient’s palm accounts for approximately 1% of the patient’s body.
While these techniques are only relatively accurate to begin with, they can also be limited by the asymmetry of injuries, patient age, and variability of opinions across different specialists. Nevertheless, they are used to assess mortality risks, define the frequency and quantity of needed procedures (IV, dressing changes, etc.), and plan surgeries.
By introducing machine learning to the burned area examination, providers can eliminate the guessing game and overcome the variability of opinions when calculating patient risks for surgical planning and following recovery. The algorithms can assess the burned surface area as well as define the burn depth to estimate the severity with high precision. This will allow the surgeons to plan tissue transplantation more accurately.
This approach was already studied and proved quite successful by Taiwanese researchers, who used artificial neural networks and reflectance spectrometry to assess the burn depth and predict patient health outcomes. The researchers created a model that was able to predict whether an injury will take more or less than 14 days to recover with 86% accuracy. This is better than the prediction power of visual examination (50–75%) but a little worse than that of Doppler flowmetry (90%). The latter, however, has a higher cost and takes more time, which makes the spectrometry based on machine learning a viable alternative.
Microsurgery: post-therapy monitoring
The road to helping patients recover successfully starts from post-surgery monitoring, which can be significantly improved with the help of machine learning, as the SilpaRamanitor app’s creators claim. This application allows detecting early anastomotic failure or thrombotic issues in patients who have undergone microsurgery.
SilpaRamanitor’s algorithms were trained on smartphone images of middle and index fingertips. Changes in their color may indicate abnormal perfusion. The algorithms categorized the captured images into three groups: normal, outflow occlusion, and inflow occlusion. If the app identifies an occlusion, it can also tag the complication’s degree as partial or complete. Remarkable, the solution achieved 94% sensitivity, 98% specificity, and 95% accuracy. And, even better, since the app can be used on any modern smartphone, it will make postoperative monitoring for patients after microsurgery feasible even in rural areas.
Measuring thrice to cut once
Information about the author


